Walk into any pharmacy and there is an entire shelf dedicated to acne soaps. Salicylic acid bars, benzoyl peroxide washes, sulfur soaps, tea tree cleansers — all promising clearer skin. Some of them genuinely help. Others are not much better than washing your face with water.
The honest answer to whether medicated soap works for acne is: it depends entirely on the active ingredient, its concentration, and — crucially — the fact that you rinse it off.
The confusing part is that “medicated soap” can mean very different things. Some products target acne bacteria, some unclog pores, some reduce oil, and some mainly reduce inflammation.
That is why the ingredient matters far more than the word “medicated” itself.
This last point is something most product labels quietly avoid discussing. A soap has seconds to minutes of skin contact before it is washed down the drain. Leave-on treatments have hours. That gap matters a lot when you are trying to clear active acne.
This guide explains the science behind each major medicated soap ingredient, what the clinical evidence shows about rinse-off products specifically, who benefits from them, and when medicated soap alone simply is not enough. No hype, no product pushing — just a clear, evidence-based picture so you can make an informed decision.
| Quick Answer — for readers in a hurry Medicated soap can help with acne — but it works best as a supportive cleansing step, not a standalone treatment. Salicylic acid and benzoyl peroxide in wash-off form are the most evidence-backed. The 2024 JAAD Acne Guidelines give benzoyl peroxide a strong recommendation and salicylic acid a conditional recommendation for acne management. Because these are rinse-off products, their contact time is short — meaning they work best alongside a leave-on treatment for moderate or persistent acne. For mild, non-inflammatory blackheads and surface oiliness, a good medicated cleanser can genuinely make a meaningful difference on its own.[1] |
Section 1: What Is Acne, and What Does Soap Need to Do to Address It?
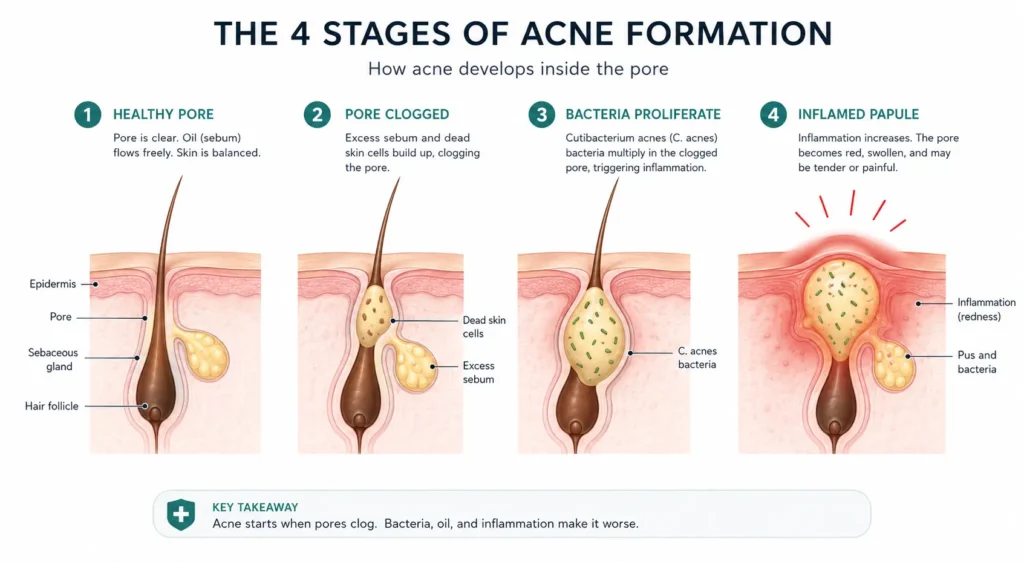
Acne is not simply a surface problem. The 2024 JAAD Guidelines describe it as ‘a chronic inflammatory skin disorder’ driven by four interconnected factors:[1]
- Excess sebum production — androgen-driven overactivity of the sebaceous glands
- Follicular hyperkeratosis — excess dead skin cells clogging the pore opening
- Cutibacterium acnes (C. acnes) proliferation — previously called Propionibacterium acnes; the bacteria that colonises the oxygen-poor, sebum-rich pore environment.
- Inflammatory immune response — the redness, swelling, and pain that follows bacterial activity
For a soap to meaningfully address acne, it needs to target at least one — ideally more — of these four pathways.
Plain soap and water addresses surface sebum and some dead skin cell accumulation.
Medicated soap adds an active pharmaceutical ingredient designed to go deeper: into the pore lining, into the bacterial environment, or into the inflammatory response itself.
Here is where the rinse-off limitation matters. The longer an active ingredient stays on skin, the more it can penetrate into the follicle and work on the underlying cause.
A leave-on salicylic acid product has all night to work. A salicylic acid soap has 30–60 seconds before it is rinsed away. This is a real pharmacokinetic constraint — not a marketing detail to dismiss.
| The skin type context matters too The pH of the soap base also affects how well it controls acne. A traditional alkaline bar soap (pH 9–10) disrupts the skin’s acid mantle and microbiome — potentially worsening the bacterial imbalance that drives acne, even if it contains an active ingredient. For this reason, medicated cleansers in liquid or syndet bar formats (pH 5.5–6.5) are generally preferable to medicated traditional bar soaps for acne-prone skin. We cover pH and the acid mantle in detail in our syndet bar science guide. |
Section 2: The Five Major Medicated Soap Ingredients — What the Evidence Shows
Below, each active ingredient is explained clearly, with the evidence for and against its use in rinse-off soap format.
Where clinical trials exist specifically for wash-off products, they are cited. Where the evidence applies primarily to leave-on formulations, that is stated honestly.
1. Salicylic Acid — The Best-Evidenced Cleanser Active
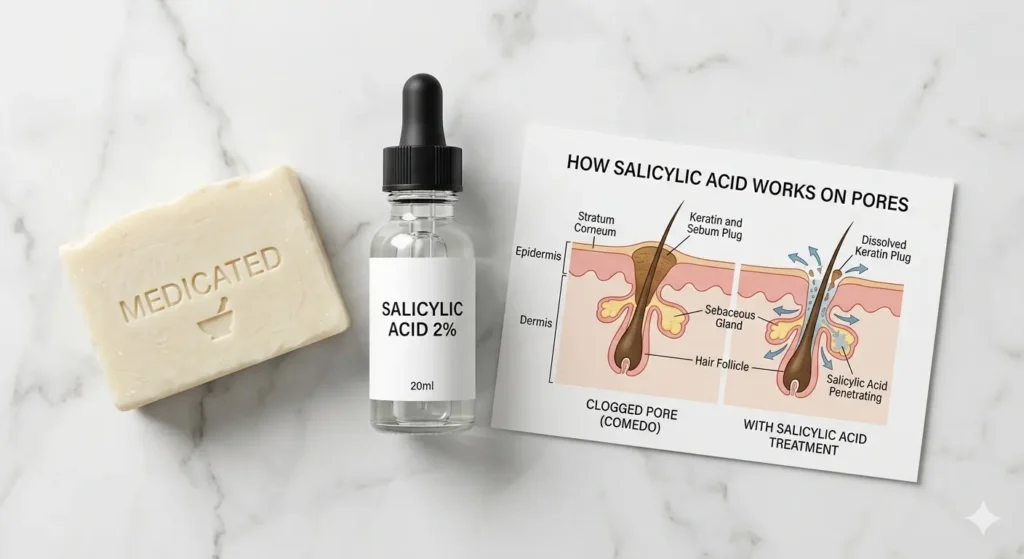
Salicylic acid (SA) is a beta-hydroxy acid (BHA) — meaning it is oil-soluble, which allows it to penetrate into sebum-filled pores rather than just working on the water-based skin surface.
This is what makes it particularly well-suited to acne: it can reach where the problem is.
Its primary mechanism is keratolysis — dissolving the dead skin cells (corneocytes) that clog pore openings and trap sebum and bacteria inside.
The 2024 JAAD Acne Vulgaris Guidelines give salicylic acid a conditional recommendation for acne management — meaning evidence supports its use, but the quality or quantity of trials is lower than for benzoyl peroxide or retinoids.[1]
A 2025 prospective clinical study (Huashan Hospital / CeraVe research, published in Wiley Journal of Cosmetic Dermatology) evaluated a salicylic acid gel over 21 days in acne patients and confirmed significant sebum reduction, reduced acne lesion counts, and improved skin barrier function — without increasing dryness or TEWL.[2]
A 2023 randomised controlled trial comparing salicylic acid to benzoyl peroxide 5% for mild-to-moderate acne found that both reduced acne severity and lesion counts to a similar degree — confirming SA is a clinically legitimate alternative for those who cannot tolerate BPO.[3]
| What salicylic acid soap is genuinely good for Blackheads (comedonal acne) — pore unclogging is where SA excels Mild inflammatory acne — reduces the blocked pore environment that bacteria thrive in Oily skin with enlarged pores — reduces surface sebum and pore appearance Daily maintenance after an active acne treatment course |
| Honest limitation Salicylic acid at 0.5–2% in a rinse-off cleanser will deliver less keratolytic effect than a leave-on 2% SA product used overnight. For stubborn or moderate acne, use SA soap as your morning cleanse alongside a leave-on SA serum or BPO treatment at night — not instead of it. |
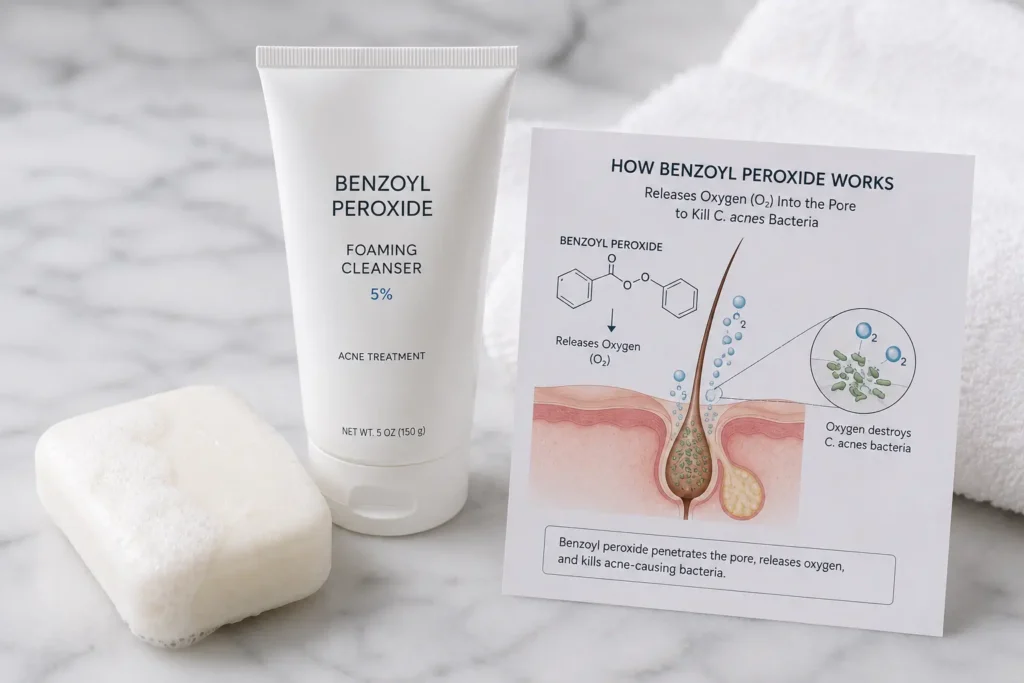
2. Benzoyl Peroxide — The Strongest Evidence, but Comes with Trade-offs
Benzoyl peroxide (BPO) is the only acne active ingredient with a strong recommendation from the 2024 JAAD Guidelines for mild-to-moderate acne — meaning multiple high-quality RCTs support its efficacy.[1]
It works by releasing oxygen inside the pore, killing C. acnes bacteria (which cannot survive in oxygen-rich environments). It also has direct anti-inflammatory and mild keratolytic effects.
Critically, BPO is one of the few topical acne agents with no documented antibiotic resistance risk — a significant advantage over topical antibiotic soaps, which contribute to the growing resistance problem. This is one reason dermatologists often pair BPO with other treatments as a resistance-prevention strategy.
A 2024 Wiley randomised study (Dal Belo et al., La Roche-Posay Research) comparing a multitargeted salicylic acid-based dermocosmetic to BPO 5% gel found both effective for mild-to-moderate acne over 15 days — but also documented BPO’s well-known side effect profile: dryness, irritation, and bleaching of fabric.[4]
For rinse-off soap formats, BPO’s irritation risk is lower than in leave-on formulations because contact time is shorter — but it also means the therapeutic effect is proportionally reduced.
One important practical note: BPO bleaches fabric. It will permanently discolour towels, pillowcases, and clothing it contacts before fully drying. Use white or designated towels when using any BPO cleanser.
| What benzoyl peroxide soap is genuinely good for Inflammatory papules and pustules — BPO’s antibacterial action directly targets C. acnes Body acne (back, chest) — where leave-on BPO is impractical, a BPO wash is the next best approach Preventing antibiotic resistance — safe long-term use without developing bacterial resistance Maintenance after prescription acne treatment — many dermatologists recommend BPO wash as ongoing maintenance |
| Honest limitation BPO washes deliver less therapeutic effect than leave-on BPO formulations. For moderate-to-severe inflammatory acne, a BPO cleanser should accompany — not replace — a leave-on BPO or retinoid treatment. Also: concentration matters. Most OTC BPO soaps range from 4% to 10%. Research suggests 2.5% BPO leave-on products are as effective as 10% with significantly less irritation — but this concentration comparison does not directly translate to rinse-off products, where higher concentration may be more appropriate to compensate for shorter contact time. |
3. Sulfur Soap — Underrated, Under-Researched, but Practically Useful
Sulfur has been used in dermatology for over a century, predating most modern acne treatments.
It works through multiple mechanisms: mild keratolysis (similar to SA), antimicrobial activity against C. acnes and Malassezia (the yeast implicated in fungal acne), and sebum-absorbing properties.
Despite its long history, modern RCT evidence for sulfur soap specifically in acne is limited — most studies are older and smaller in scale.
Its main practical advantage is its suitability for sensitive and acne-prone skin that cannot tolerate BPO or high-concentration SA.
It is less irritating than both, and at 3–10% concentration in soap, it provides a gentler antimicrobial cleansing action.
Sulfur soap is also effective for seborrheic dermatitis and rosacea — skin conditions that often accompany or mimic acne — making it useful when the diagnosis is unclear.
| Key limitation: the smell Sulfur has a characteristic egg-like odour that many users find off-putting. Modern formulations have improved significantly, but if scent sensitivity is a concern, SA or BPO cleansers are more comfortable options. |
4. Zinc Pyrithione (ZnP) Soap — Specific Use Cases, Not General Acne
Zinc pyrithione (ZnP) is primarily an antifungal agent — it kills Malassezia yeast, the organism responsible for dandruff, seborrheic dermatitis, and fungal acne (pityrosporum folliculitis).
The distinction matters enormously: zinc pyrithione does not significantly help with standard bacterial acne (C. acnes-driven) and should not be the first choice for typical pimples and blackheads.[5]
Where ZnP soap is genuinely useful: when your ‘acne’ is actually fungal folliculitis — a condition that looks identical to acne but is driven by Malassezia yeast rather than C. acnes.
Fungal acne typically presents as small, uniform, itchy papules on the chest, back, or forehead, often worsening in humid conditions or after antibiotic use.
A dermatologist can distinguish the two with a simple skin scraping. If ZnP soap reduces your breakouts when conventional acne treatments failed, fungal acne is a strong possibility.
ZnP at 2% concentration is FDA-recognised as safe and effective in rinse-off products for seborrheic dermatitis and dandruff.[6]
The EU has restricted ZnP in cosmetics due to environmental concerns, favouring piroctone olamine as an alternative — though in the US, ZnP remains the standard of care for seborrheic dermatitis maintenance.
5. Tea Tree Oil and Herbal Actives — Supported but as Complementary Options
Tea tree oil (terpinen-4-ol as the primary active) has documented antimicrobial activity against C. acnes and has been compared to benzoyl peroxide in acne studies.
A comparative review found a 5% tea tree oil gel comparable to benzoyl peroxide for reducing mild-to-moderate acne lesions, with fewer side effects.[7]
In soap format, Tea Tree Oil concentration is typically lower than 5% and the rinse-off limitation applies — but TTO soaps are a reasonable option for those who react to BPO or SA.
Neem’s active compounds (nimbidin, azadirachtin) have documented antibacterial activity against S. aureus and anti-inflammatory properties.[8]
Combined with tea tree oil, they form one of the stronger herbal-based antimicrobial soap options.
For the full breakdown of herbal ingredients and their evidence levels, read our herbal soap benefits guide.
Section 3: The Complete Comparison — All Five Actives Side by Side
| Ingredient | Acne Type | Evidence | Best For | Key Limitation |
|---|---|---|---|---|
| Salicylic Acid | Comedonal and mild inflammatory acne | Strong; supported by multiple acne studies | Blackheads, oily skin, clogged pores | Rinse-off format reduces pore contact compared with leave-on products. |
| Benzoyl Peroxide (BPO) | Inflammatory papules and pustules | Strongest overall evidence among common acne cleansers | Red pimples, bacterial acne, body acne | Can bleach fabric and cause dryness or peeling. |
| Sulfur | Mild acne, oily skin, seborrhoeic dermatitis overlap | Moderate; fewer modern acne-specific trials | Sensitive oily skin and mild acne | Strong smell and limited modern evidence. |
| Zinc Pyrithione (ZnP) | Fungal acne only | Moderate for fungal conditions | Itchy chest/back breakouts | Not useful for standard C. acnes acne. |
| Tea Tree / Neem | Mild bacterial acne | Moderate; tea tree has stronger acne evidence than neem | People avoiding stronger medicated cleansers | Soap formulas often use lower concentrations. |
Section 4: The Rinse-Off Problem — Why Medicated Soap Alone Often Isn’t Enough
This is the most important section in this article — and the one most acne soap labels never mention.
Medicated soap is a rinse-off product. That means its active ingredient has contact with your skin for roughly 30–90 seconds before it is washed away.
Most pharmacokinetic research on topical acne actives is conducted on leave-on formulations — creams, gels, and serums that stay on the skin for hours. The evidence from those studies does not directly transfer to a 60-second wash.
That said, this does not mean medicated soap is worthless — far from it. Here is how to think about what it can and cannot do:
What Medicated Soap Can — and Cannot — Realistically Do
Medicated soap can support acne control, especially for oily skin and mild breakouts, but it is not a complete replacement for a full acne treatment routine.
✓ What Medicated Soap CAN Do
- Remove excess oil, debris, and dead skin cells from the skin surface.
- Reduce surface C. acnes bacteria during cleansing.
- Help exfoliate pore openings, especially with salicylic acid cleansers.
- Prepare skin for leave-on acne treatments by removing excess oil buildup.
- Support body acne management where leave-on products are inconvenient.
- Help maintain results after stronger acne treatment phases.
✗ What Medicated Soap CANNOT Do Alone
- Clear moderate-to-severe inflammatory acne alone.
- Replace leave-on acne medications for persistent acne.
- Penetrate deeply into follicles during short wash contact time.
- Prevent all future breakouts without a broader skincare routine.
- Treat hormonal, cystic, or nodular acne effectively on its own.
- Replace dermatologist-prescribed treatment when acne becomes severe or scarring.
Section 5: Who Actually Benefits from Medicated Soap?
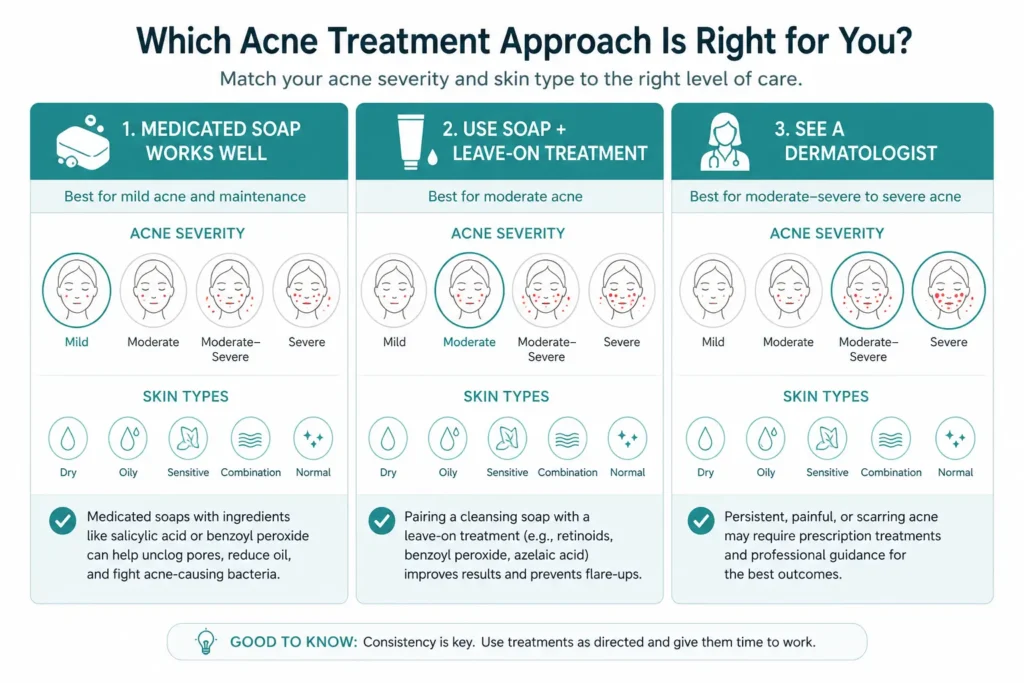
Medicated soap works well as a primary tool for:
- Mild, non-inflammatory acne — blackheads and whiteheads with minimal redness. SA soap used twice daily can genuinely keep mild comedonal acne under control without additional treatment.
- Body acne prevention and maintenance — back and chest acne responds particularly well to BPO or SA washes because leave-on products are impractical to apply on large body surface areas and dry out clothing.
- Oily, congestion-prone skin in humid climates — daily SA cleansing reduces the sebum accumulation that creates the environment for acne without over-drying the skin.
- Post-treatment maintenance — after completing a prescription acne course, a SA or BPO medicated wash helps prevent relapse. The 2023 J Drugs Dermatol study found that a salicylic acid-containing dermocosmetic ‘allowed a significant reduction of acne relapse compared with vehicle after 3 months of follow-up’.[9]
Medicated soap is not enough alone for:
- Moderate-to-severe inflammatory acne — papules, pustules, nodules. The 2024 JAAD guidelines recommend combined topical therapy (BPO + retinoid or antibiotic) for moderate acne. A cleanser alone, however good, does not meet this standard.[1]
- Hormonal or cystic acne — deep, painful nodules driven by androgen fluctuations require systemic treatment (oral contraceptives, spironolactone, isotretinoin). No topical soap can address the hormonal driver.
- Acne causing scarring or significant psychosocial distress — the JAAD guidelines specifically note that acne causing scarring or emotional burden warrants oral isotretinoin consideration. At this severity level, self-treating with OTC soap is not appropriate.
Section 6: How to Use Medicated Soap Correctly — Maximising Contact Time
The contact time limitation is real, but you can partially offset it with the right technique. Most people lather and rinse in under 20 seconds. Some actives benefit significantly from a longer contact period.
- Wet skin with lukewarm water (not hot — hot water increases TEWL and skin reactivity, making medicated actives more irritating).
- Lather the product in your palms first before applying to skin. This distributes the active more evenly than applying bar directly.
- Apply to skin and leave for 60–90 seconds before rinsing. For BPO washes and ZnP soap particularly, manufacturers often recommend 30–60 seconds of contact time. Use this time to brush teeth or wash another body part.
- Rinse thoroughly with lukewarm water. Any remaining active — particularly BPO — can irritate if it sits on the skin’s edges, hairline, or neck.
- Pat dry gently with a dedicated white towel (if using BPO) or a soft cloth. Do not rub.
- Apply leave-on treatment immediately while skin is still slightly damp — this is when active ingredients absorb most effectively.
| The routine that actually works for mild-to-moderate acne Morning: medicated SA or BPO cleanser → lightweight moisturiser → SPF 30+ (non-comedogenic) Evening: medicated cleanser → leave-on treatment (SA serum, retinol, BPO gel, or prescription retinoid depending on severity) → lightweight moisturiser The cleanser prepares the skin; the leave-on product does the heavy lifting. This is the combination most dermatologists recommend for mild-to-moderate acne. |
Section 7: What to Avoid in an Acne Soap — Ingredients That Make Things Worse
Not every soap labelled ‘for acne’ is formulated well. Some contain ingredients that actively worsen the conditions that drive acne breakouts.
| Avoid these in any acne soap Coconut oil or heavy plant oils in the base — highly comedogenic; will clog pores regardless of what active is present Synthetic fragrance / parfum — a top allergen and inflammatory trigger; can worsen inflammatory acne and cause contact dermatitis SLS at high concentration — over-strips sebum and disrupts the skin microbiome, triggering rebound oil overproduction Triclosan — FDA-banned from US consumer rinse-off products; no proven benefit over regular soap for acne; antibiotic resistance risk Alcohol denat. near the top of the INCI list — drying and barrier-disruptive; increases sensitivity and makes acne treatments more irritating Full ingredient avoidance guide with clinical evidence for each: Soap Ingredients to Avoid for Sensitive Skin. |
Signs Your Acne Soap May Be Too Harsh
- Burning or stinging after washing
- Skin feels tight or squeaky-clean
- Red flaky patches
- Peeling around the mouth or nose
- Increased oiliness after over-cleansing
- Worsening irritation after repeated use
More acne medication does not always mean better acne control. Over-drying the skin barrier can sometimes worsen irritation and rebound oil production.
For detailed explanation read whether medicated soap can damage the skin barrier.
Helpful Medicated Cleansers Worth Considering
The best medicated cleanser depends on the type of acne you actually have. Inflamed red pimples, blackheads, oily skin, and sensitive acne-prone skin often respond better to different active ingredients.
Section 8: People Also Ask — Medicated Soap Questions Answered
Does medicated soap really clear acne?
For mild acne — especially blackheads and surface congestion — yes, a well-formulated SA or BPO cleanser used consistently twice daily can produce meaningful improvement.
For moderate-to-severe inflammatory acne, medicated soap is an important part of the routine but not sufficient on its own.
The 2024 JAAD guidelines are clear that moderate acne requires combined topical therapy.[1]
Think of medicated soap as a foundation — useful and necessary, but not a complete structure.
Which ingredient is best in acne soap — salicylic acid or benzoyl peroxide?
It depends on your acne type.
Salicylic acid is better for comedonal acne (blackheads, whiteheads, clogged pores) because it is oil-soluble and can penetrate into the pore lining.
Benzoyl peroxide is better for inflammatory acne (red papules, pustules) because it directly kills C. acnes bacteria.
The 2023 RCT that compared them found similar overall efficacy for mild-to-moderate mixed acne[3] — meaning if you are unsure, either is a reasonable starting point.
If you react badly to BPO (common: dryness, bleaching), SA is the better alternative. If blackheads are your main concern, SA leads. If red, angry pimples are the issue, BPO leads.
How long does it take for acne soap to work?
Realistic timelines: surface sebum and congestion reduction — noticeable within 1–2 weeks of twice-daily use.
Reduction in active inflammatory lesions — 4–8 weeks of consistent use.
Significant overall skin clearance — 8–12 weeks, particularly for SA-based cleansers.
The 2025 CeraVe/Fudan University clinical study saw meaningful sebum reduction and lesion improvement within 21 days of SA gel use[2] — but that was a leave-on product, not a rinse-off soap. Expect soap timelines to be at the longer end.
Can I use medicated acne soap every day?
Most SA soaps (0.5–2%) and BPO washes (4–10%) are formulated for daily use — typically twice daily (morning and evening).
Start with once daily and observe skin tolerance for the first week. If dryness, peeling, or irritation develops, reduce frequency and add a non-comedogenic moisturiser.
Both SA and BPO can cause initial dryness — this typically settles within 2–3 weeks as skin adjusts.
Do not skip moisturiser when using medicated cleansers — moisturising after cleansing is a core AAD recommendation for acne management.
Is medicated soap safe for sensitive skin?
Medicated soap for sensitive-acne-prone skin requires careful ingredient selection.
Sulfur at 3–5% is the gentlest option. Salicylic acid at 0.5% is better tolerated than 2% for sensitive skin.
Avoid BPO if you have rosacea or reactive skin — its oxidising mechanism is more likely to trigger irritation.
Any medicated soap for sensitive skin should also be: fragrance-free, SLS-free, pH-appropriate (6.5 or lower), and ideally in a syndet or glycerin base.
For guidance on the base, see our glycerin soap vs regular soap guide.
What is the difference between medicated soap and a face wash for acne?
Functionally, very little — both are rinse-off cleansers delivering an active ingredient.
The meaningful differences are:
(1) base pH — a bar soap typically has higher pH (9–10) unless it is a syndet bar, while liquid face washes are typically pH 5.5–7;
(2) additional ingredients — liquid cleansers can incorporate humectants and emollients that bar soaps cannot easily include due to saponification chemistry;
(3) texture preference — purely personal. For acne management, a medicated liquid cleanser or syndet bar in the appropriate pH range is generally preferable to a traditional bar soap, even if both contain the same active ingredient.
When should I see a dermatologist instead of using OTC acne soap?
See a dermatologist if:
your acne involves nodules or cysts (painful, deep lumps); if OTC treatment has not improved acne meaningfully after 8–12 weeks;
if acne is causing scarring or significant emotional distress;
if breakouts are primarily hormonal (cyclical, along the jawline, chin, or lower face in adult women);
or if you are uncertain whether your breakouts are acne at all — fungal acne, perioral dermatitis, and rosacea all look similar and require different treatment.
The 2024 JAAD guidelines explicitly state that acne causing scarring or psychosocial burden warrants ‘strong recommendation’ for isotretinoin consideration — well beyond what any OTC soap can address.[1]
Section 9: Related Guides — The Full Skin Health Series
This article is part of skin health series. Each guide is cross-linked throughout where it is most relevant. Full navigation:
- Types of Soap and Their Benefits for Skin — Complete Guide — all soap formats including medicated, glycerin, syndet, and herbal explained
- Soap Ingredients to Avoid for Sensitive Skin — full evidence-backed avoidance list with printable checklist; includes ingredients that worsen acne
- Glycerin Soap vs Regular Soap for Skin — why base formulation matters as much as the active ingredient
- What Is a Syndet Bar? The Science Behind pH-Balanced Soap — why pH-balanced bars are better vehicles for acne actives than traditional alkaline soap
- Herbal Soap Benefits for Skin: 8 Ingredients Backed by Science — tea tree oil, neem, turmeric evidence for acne; full clinical breakdown
- Liquid Soap vs Bar Soap: Which Is Better for Skin? — why format affects how well medicated actives deliver at the skin surface
Sources & References
Superscript citation numbers throughout this article link directly to their source. Full references below.
- [1] Reynolds RV et al. Guidelines of care for the management of acne vulgaris. J Am Acad Dermatol. 2024 May;90(5):1006.e1-1006.e30. DOI: 10.1016/j.jaad.2023.12.017. PubMed PMID 38300170.
- [2] Liu Y et al. Clinical Efficacy of a Salicylic Acid-Containing Gel on Acne Management and Skin Barrier Function: A 21-Day Prospective Study. Wiley J Cosmet Dermatol. 2025. PMC12274963.
- [3] Salicylic acid versus benzoyl peroxide 5% for the treatment of acne — randomised controlled trial summary. Examine.com research feed, December 2023.
- [4] Dal Belo SE et al. Efficacy of a multitargeted, salicylic acid-based dermocosmetic cream compared to benzoyl peroxide 5% in acne vulgaris. J Cosmet Dermatol (Wiley). 2024 Mar;23(3):891-897. DOI: 10.1111/jocd.16052. PMID 37941097.
- [5] Mangion SE, Holmes AM, Roberts MS. Targeted Delivery of Zinc Pyrithione to Skin Epithelia. Int J Mol Sci. 2021;22(18):9730. PMC8465279.
- [6] FDA DailyMed — Zinc Pyrithione Soap OTC label. FDA-recognised safe and effective for dandruff and seborrhoeic dermatitis at 2% rinse-off concentration.
- [7] Treatment of acne with tea tree oil (melaleuca) products: A review of efficacy, tolerability and potential modes of action. International Journal of Antimicrobial Agents. ScienceDirect. 2015.
- [8] Formulation and Evaluation of Turmeric and Neem-Based Topical Nanoemulgel against Microbial Infection. MDPI Gels. 2024. PMC11431516.
- [9] Khammari A et al. A Salicylic Acid-Based Dermocosmetic as Adjunct to BPO and Maintenance Post-BPO for Mild-to-Moderate Acne. J Drugs Dermatol. 2023;22(12):1172-1177. DOI: 10.36849/JDD.7449. PMID 38051857.
2025 HealthSolutionBlog.com. For educational and informational purposes only. This article does not constitute medical advice. For persistent, moderate, or severe acne, consult a board-certified dermatologist.




2 thoughts on “Medicated Soap for Acne: Does It Actually Work? A Dermatology-Backed Answer”