If you are stuck, “How does HIV affect/weaken your immune system” then you are in the right place. In this article, you will learn about HIV, the replication cycle of HIV, its pathogenicity, symptoms, and opportunistic diseases step by step, each step with visuals illustrations, and pictures.
Before going to the replication of HIV, first, let’s talk about this virus generally.
Let me ask you,
Do you know the abbreviation of HIV and what it means?
A little.
Okay, let me tell you.
HIV stands for
H Human
I Immune deficiency
V Virus
Coming to the second part of the question, “and what it means,” it means the weaker and lower activity of the immune system against foreign pathogens due to this HIV virus attack because HIV weakens the immune system.
What disease does this virus cause?

You are asking about the pathogenicity of HIV. AIDS is a very dangerous disease caused by this virus, in which the immune system is profusely suppressed by HIV and other opportunistic diseases.
The word AIDS stands for
A Acquired
I Immune
D Deficiency
S Syndrome
Why is it called “acquired immune deficiency” and “syndrome”?
The “Acquired” means that it is caused by the “Human immune deficiency virus (HIV)” and as already discussed this virus dangerously damages the immune system while the “Syndrome” means the other complications that arise due to this disease (AIDS) which we will discuss in “opportunistic diseases” later.
Tell me, Is this an RNA virus or a DNA virus?

HIV belongs to retrovirus which means it is an RNA virus.
If this is a retrovirus (RNA virus) then how does it take to control the host cells?
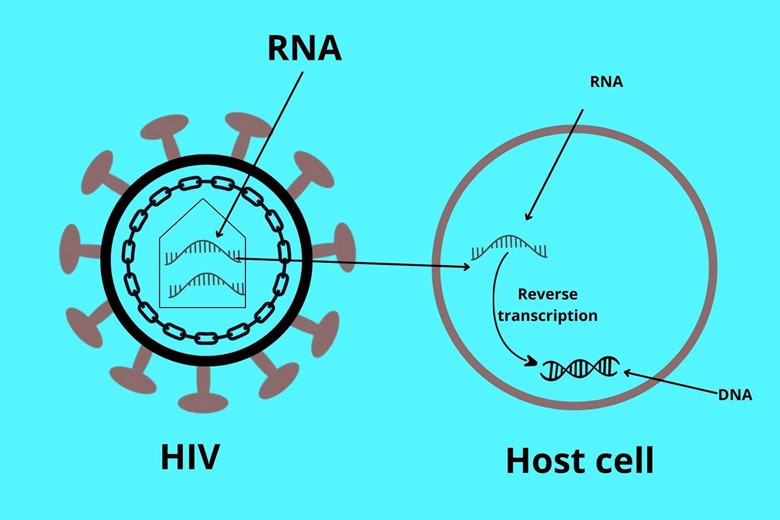
This is a good question. DNA is the main genetic material that can code for amino acids and can take the host biosynthetic machinery to overtake for their use, but HIV is a retrovirus so after entry into the host cell it reverses its genetic material (RNA) to DNA by the process of reverse transcription.
Before going to the replication cycle, let’s explain the structure of HIV.
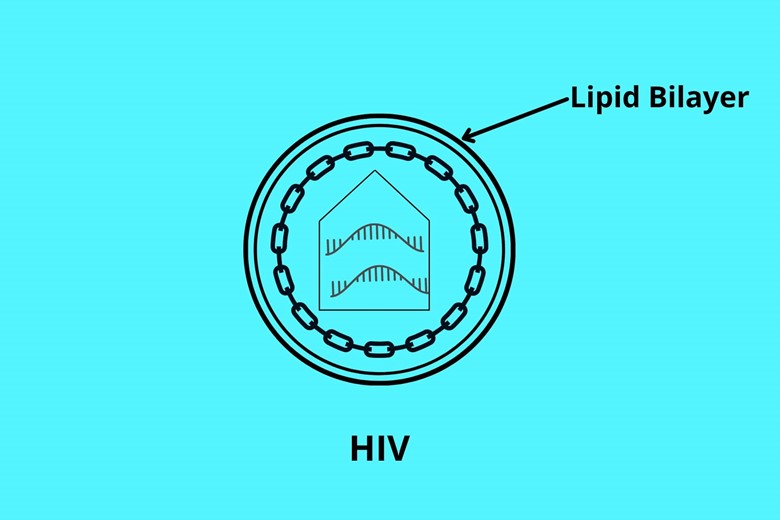
HIV lives in a lipid bilayer bubble where it is protected.
But how does HIV make a lipid bilayer because it has no DNA so it codes for a lipid bilayer?
This is also a very good question. As already discussed this virus is a retrovirus and lives in a host so it steals the part of the lipid bilayer and makes a bubble for their protection.
The lipid bilayer has special proteins called envelope proteins which help them in attachment to the host cell. Let me explain them one by one.
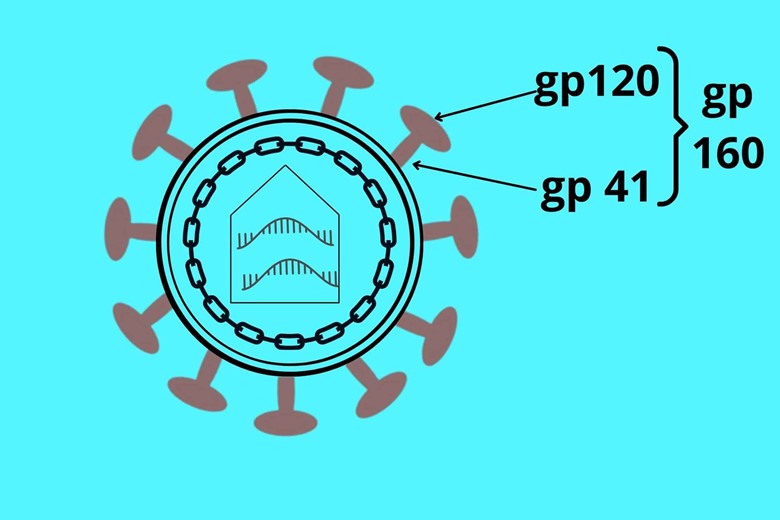
The lipid bilayer has a special trans protein called gp 41 (gp stands for glycoprotein). At the top of trans protein (gp 41), there is another docking protein called gp 120. The gp 120 is called a docking protein because it adjusts to the target cell receptor. The whole complex protein (gp 41 + gp 120) is called gp 160.
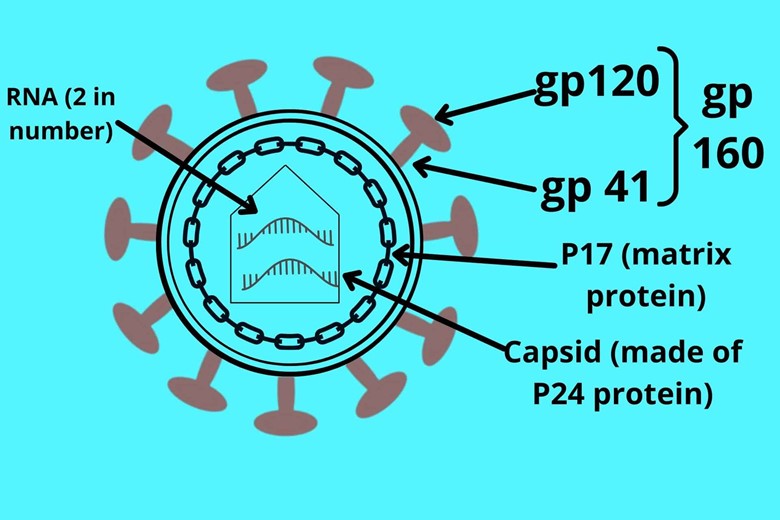
Under envelope protein, there is another protein layer called matrix protein or p17 where capsid is present. The capsid has 20 sides due to which it is called icosahedral where the RNA resides. The sides of the icosahedral capsid are made of p24 protein. The numbers are given due to their molecular weight that’s why it is random.
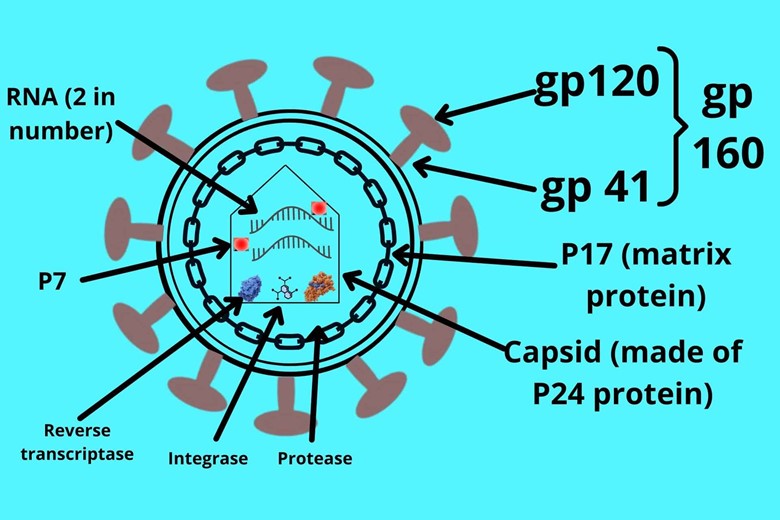
Inside the capsid, two identical RNA copies with p7 protein are present. HIV needs special enzymes for the attack that it carries with itself and those are reverse transcriptase, integrase, and protease.
Now coming to the replication of HIV, Which cell in the body does the virus infect?
HIV loves to infect with Cd4 positive cells because gp 120 loves to bind with cd4 positive cells. The cd4-positive cells in our body are T-helper cells, monocytes, macrophages (activated monocytes in tissue), microglia (macrophages in CNS), Langerhans (dendritic cell under the skin), follicular dendritic cells in the spleen and lymph nodes.
But why these immune cells don’t attack HIV because immune cells are for killing invading particles?
Good question. As every invading virus or particle or germ has target cells they infect. The target cells of HIV are CD+ positive T-helper cells while T-helper cells activate the advanced immune system for advanced action to kill the invading pathogen but here the T-helper cells are killed by HIV which then cannot activate the advanced immune system leading to the failure of the human immune system. At the start, the symptoms are not significantly visible but as the T-helper cells get low and the immune system is weakened then the symptoms start visible.
So how does HIV kill T-cells??
Let’s explain it.
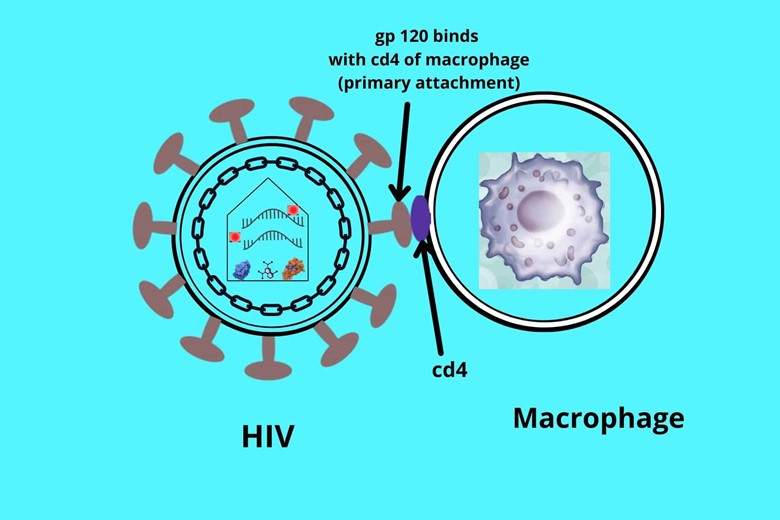
Let’s take the CD4-positive macrophage cell as shown in the picture. Initially, in most cases of naturally acquired AIDS, the virus infects the macrophages because these cells have CCR5 as a secondary co-receptor and HIV has an attraction to bind with CCR5 but after many generations, some strains are produced which can bind with CXCR4 co-receptor making the virus more dangerous. The binding starts with gp 120 of HIV which gets attached with the cd4 of macrophage. This attachment is called a primary attachment but this is not enough attachment due to this the virus will form other attachments too.
But why the cell has a co-receptor for the virus?
This co-receptor is not for the virus, it is a receptor for chemokines. Chemokines are a group of cytokines whose function is signaling to the cell after secretion by the cell.
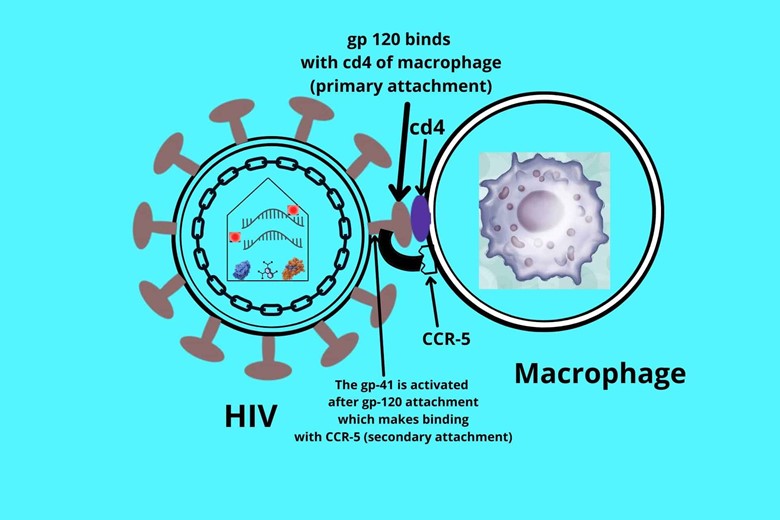
After the primary attachment, the gp 120 undergoes conformational changes which activate their other active site that bind with the co-receptor of the cell which is called chemokine receptor-5 (CCR5) in the case of macrophage cell
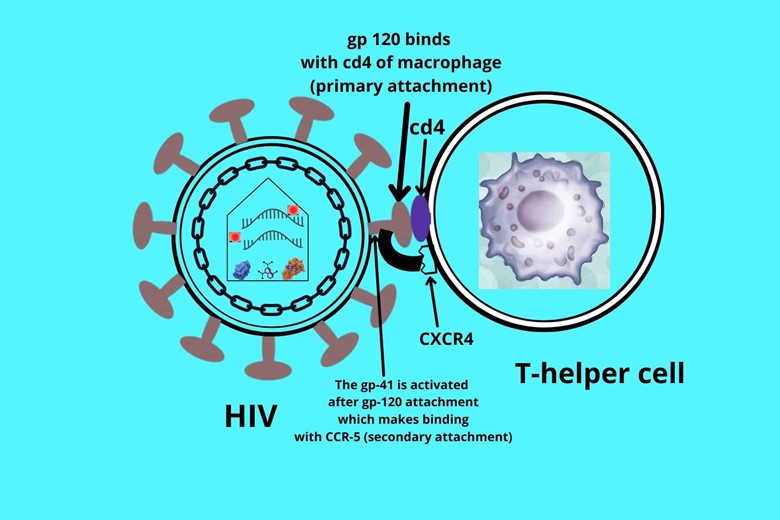
but in the case of T-helper cells, the binding is a little different because of different co-receptors i.e. CXCR4. The co-receptor attachment is called secondary attachment.
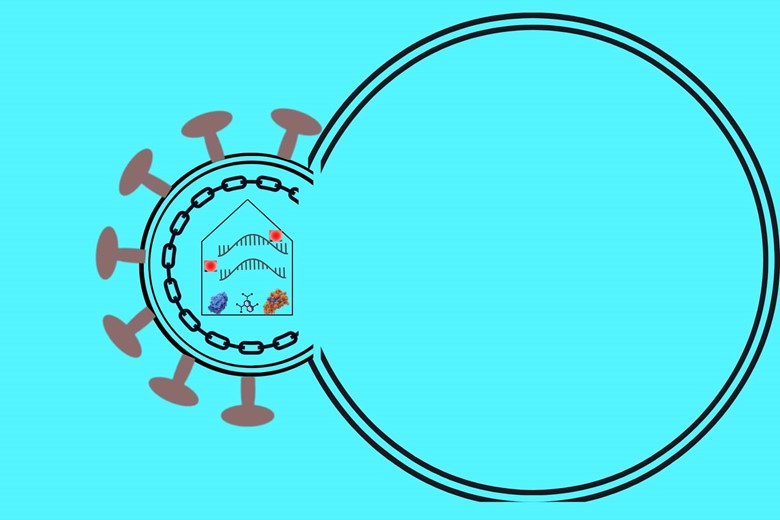
After the primary and secondary attachment, the gp 41 is activated and undergoes the changes that will hook the target cell (cd4+ cell). The hook then pulls the virus and targets cells towards themselves and both gp 41 and the target cell membrane are lipid bilayers so they will fuse.
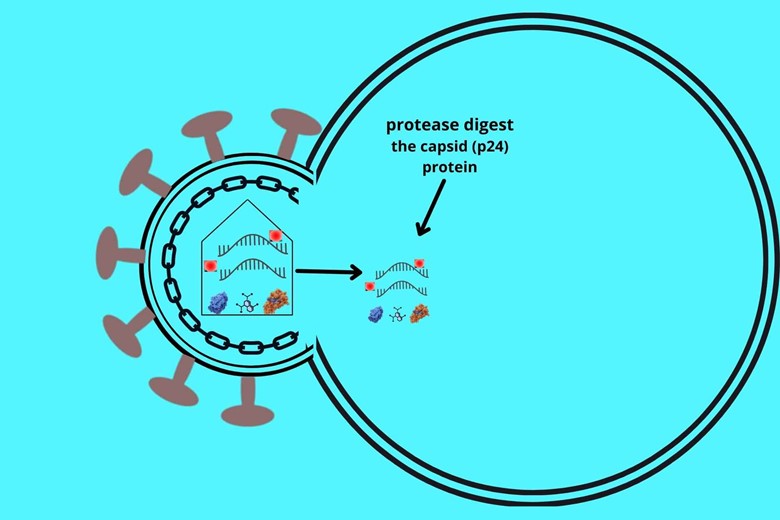
In the next step, the lipid bilayer of both the virus and target cell fuse together, and the virus then inject its core protein i.e. capsid with RNA and enzymes into the target cell of the host. After entry to the host cell, the proteases of the host cell come and dissolve the capsid protein i.e. p24. Now the genetic material and enzymes of the virus are in the cytoplasm of the host target cell.
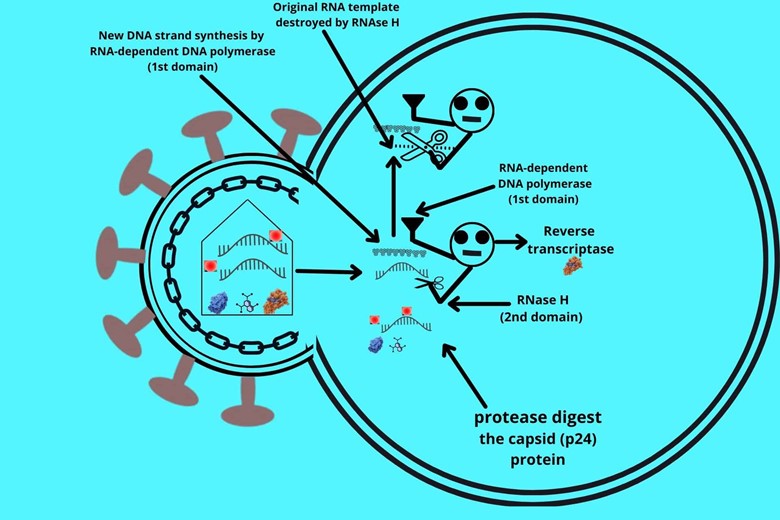
The first action in the enzymes is reverse transcriptase which has two domains. One domain is RNA-dependent DNA polymerase and the other domain is RNase H. The RNA-dependent DNA polymerase first reads the RNA and makes a new complementary DNA. The RNase H will destroy and digest the original template of HIV RNA.
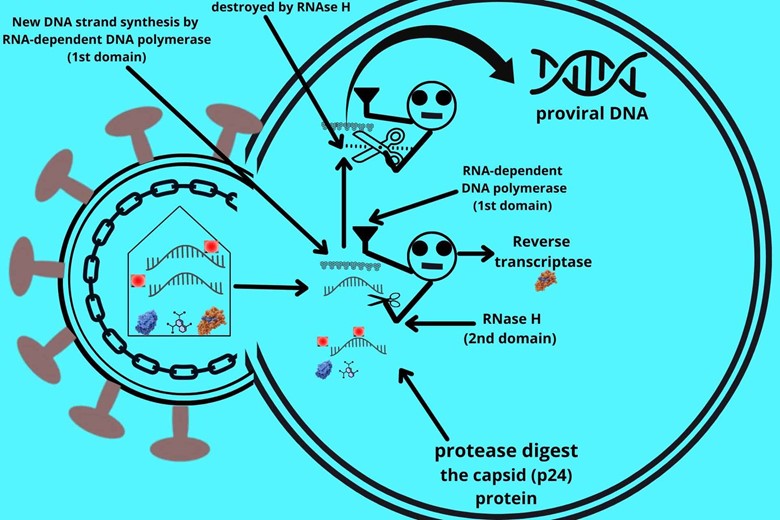
The DNA is still single-stranded due to which enzymes will come and make a new complementary DNA strand to make a double-stranded DNA. Now this double-stranded DNA is called proviral DNA.
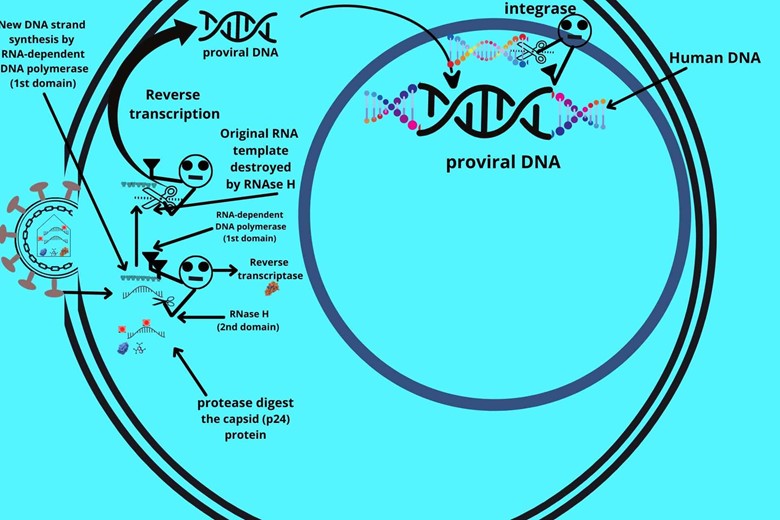
The proviral DNA is then carried to the nucleus where the integrase enzyme is activated. The integrase enzyme has two domains. One domain will cut the human DNA and the other domain glue the proviral DNA into it. The viral DNA is integrated into human DNA and unfortunately, once this HIV DNA is integrated into human DNA it becomes their part permanently that’s why it is difficult to cure this disease. This proviral DNA can only be removed when the human cell is destroyed.
Let me explain to you how proviral DNA integrates into human DNA?
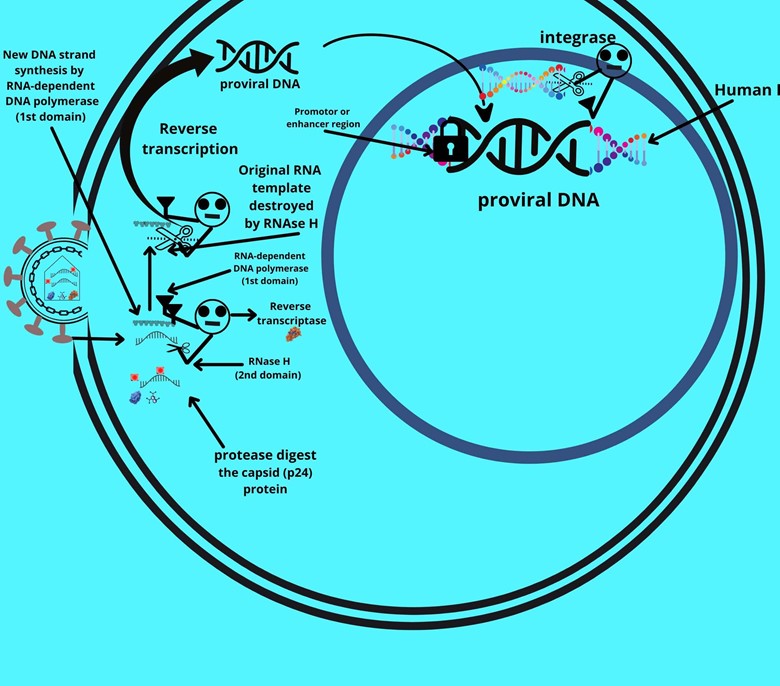
The proviral DNA has sticky ends which are called long terminal repeats (LTR) because the nucleotide sequence is multiply repeated here. The LTR sticks the ends of proviral DNA to human DNA and also it has a promotor or enhancer region. The promotor region is activated by their special transcription factor which upon activation starts the multiplication of DNA, unfortunately, our body produces transcription factor for itself which activates this proviral promoter region and starts their copying.
Do you remember that HIV has proteins and enzymes that are necessary for its complete structure?
We discussed that was
P17 (matrix protein)
P24 (Capsid protein)
P7 (nucleocapsid protein)
Yes. That’s correct.
Now the virus needs these proteins to make a new virus. For this proviral DNA has different genes which will make these proteins after expression.
How?
As already discussed the transcription factor activates the promotor region of proviral DNA, and the genes are activated.
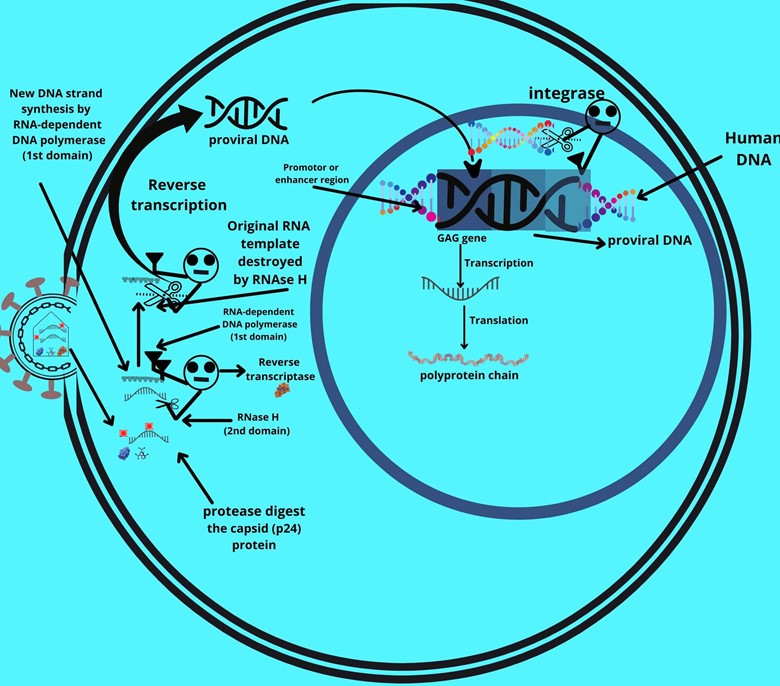
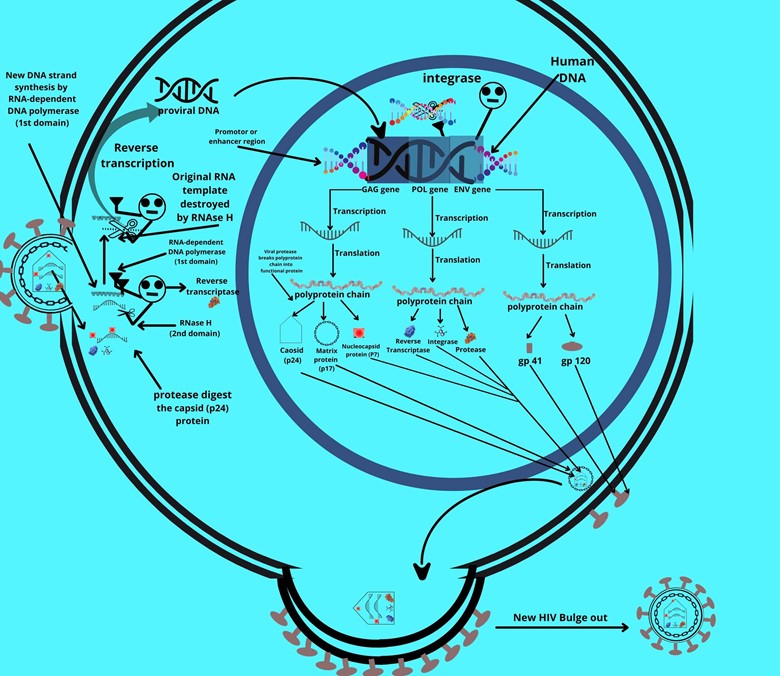
There is a gene called the GAG gene which after activation transcribes mRNA. The mRNA then synthesizes a non-functional polyprotein chain.
What is meant by a polyprotein chain?
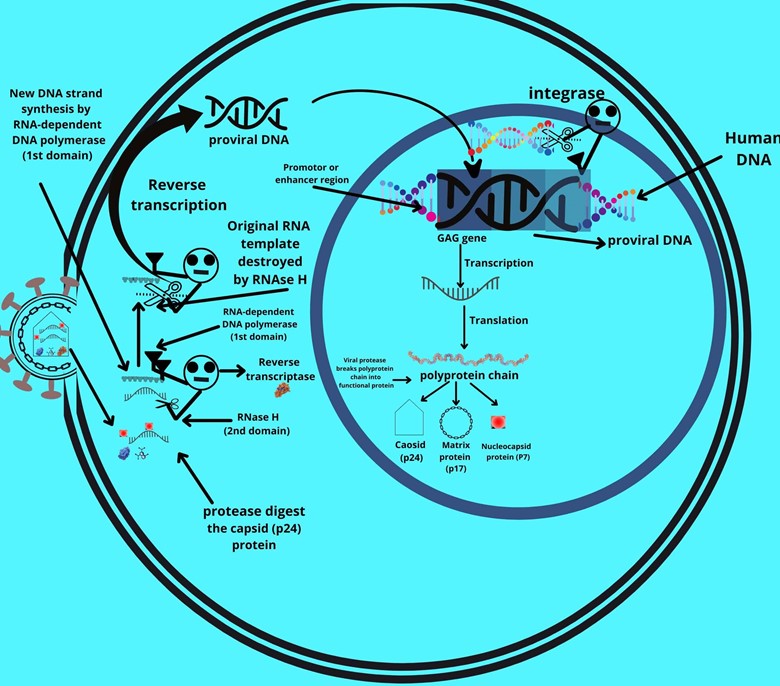
The polyprotein chain means that it contains more than one polypeptide sequence which is then cut into functional p24, p17, and p7 proteins by viral protease enzyme.
But what about the “reverse transcriptase, integrase, and protease enzymes”?
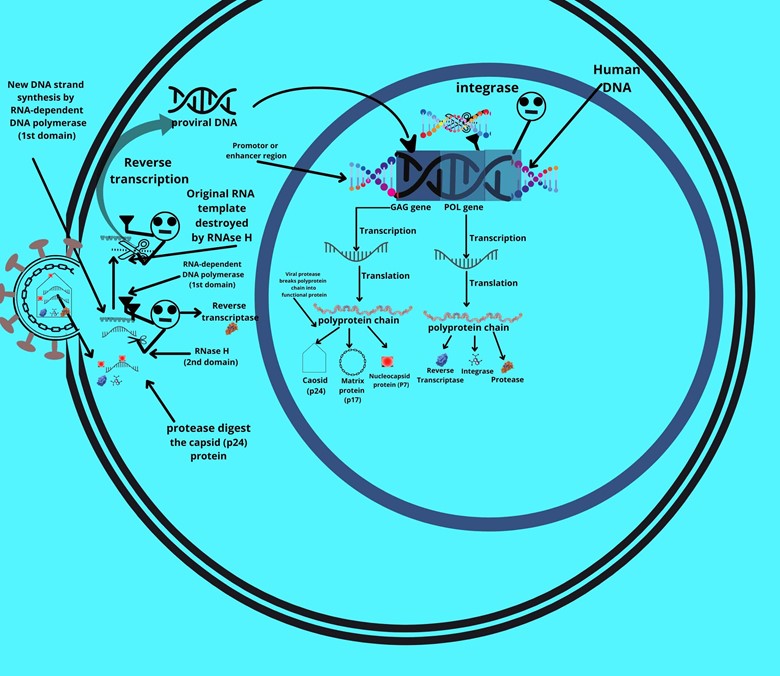
There is another gene called the POL gene which is present in proviral DNA. Upon activation, it also transcribes to mRNA, and again mRNA synthesizes a non-functional polyprotein chain. The chain is again cut by viral proteases but this time into different products i.e. reverse transcriptase, integrase, and protease.
What remains?
The gp 160 protein (gp 41 + gp 120).
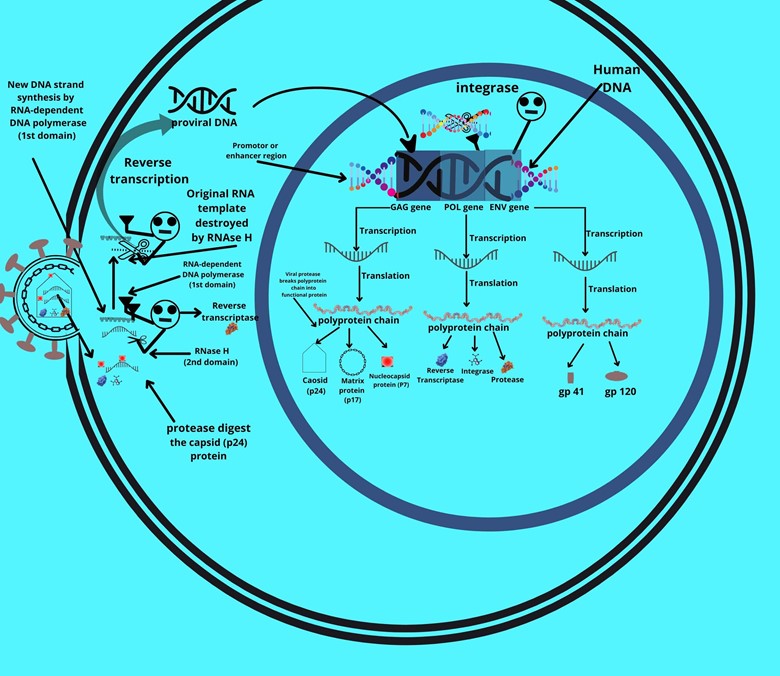
Exactly. The third gene is called the ENV gene which upon activation results in the transcription of mRNA which will synthesize a non-functional polyprotein chain. The polyprotein, this time is, unfortunately, cut by human cellular proteases into gp 41 and gp 120 (gp 160). This forms the envelope of the virus.
These three genes are present in all HIV.
These three genes also synthesize other six types of protein.
How? Because we have read one gene for one protein.
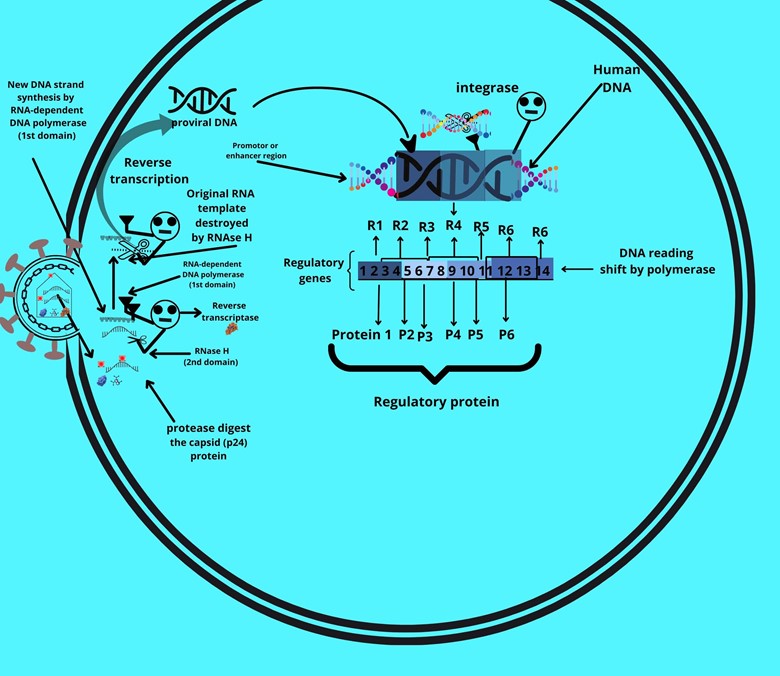
The HIV viral genome has a reading shift by polymerase which means that sometimes the polymerase reads the sequence one way and the other time it reads another way. The protein made by this method is called regulatory proteins while the genes are called regulatory genes.
For example. In the above picture, reading 1 will transcribe one protein while reading 2 will transcribe the other protein, and so on.
Can you give an example of regulatory genes and their regulatory proteins?
Yes.
Following are the six different regulatory genes and their regulatory proteins
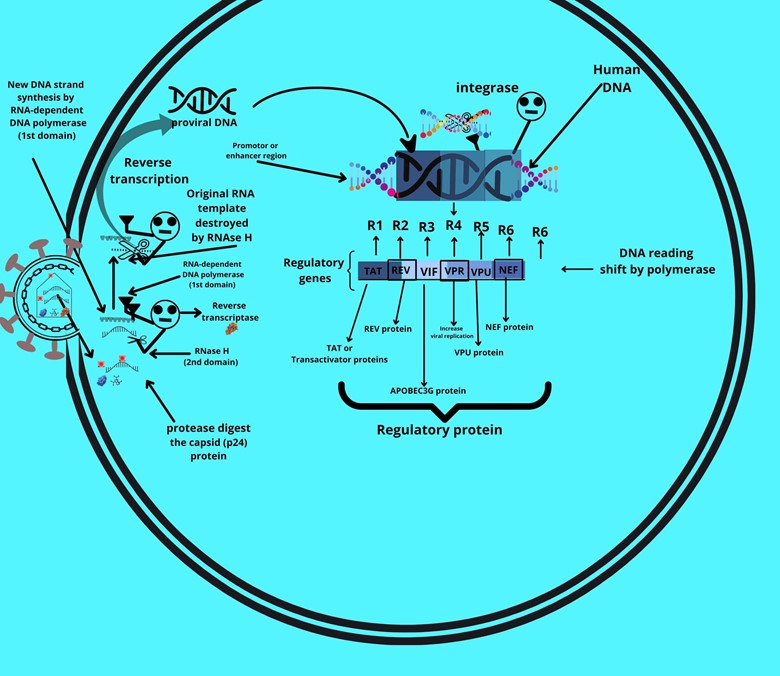
- TAT or Transactivator gene produces TAT or Transactivator proteins which will go to LTR (Long terminal repeats) where it binds with the promotor region and amplifies the viral transcription more than a thousand times.
- REV gene produces a REV protein that will take the mRNA of viral DNA from the nucleus and carry it to the cytoplasm efficiently so that it amplifies the mRNA transcription and produces more viruses.
- VIF or viral infectivity factor synthesizes a protein that damages the APOBEC3G protein. The APOBEC3G protein is normally present in human blood and its function is to damage and destroy any incoming viral DNA so the HIV shift reads a gene that will produce the product which will damage and destroy the APOBEC3G protein.
- VPR protein, about VPR protein we don’t know but it increases viral replication.
- VPU protein increases viral release by destroying tetherin. Tetherin protein does not allow the release of viruses in the body.
- NEF protein of the virus suppresses the MHC class I molecule. When there is an entry of a virus or foreign protein the MHC-I molecule takes the part of the entered virus or protein and presents it to the T-cytotoxic cell (TCT). The T-cytotoxic cell then destroys the whole cell including the virus or foreign protein. This NEF protein is a defensive mechanism of the virus that suppresses the MHC-I molecule so that the cell cannot report the presence of the virus or foreign protein to T-cytotoxic cells and replicate themselves safely.
Now it’s time to assemble these proteins and make a new virus.
The gp 41 and gp 120 proteins move to the host cell membrane where they get attached. Then the matrix protein (P17) comes and attaches under it. For the genome of the virus i.e. RNA,
I will ask a question from you.
Do you remember the integration of viral DNA to host DNA?
Yes.
Here is the point, if the whole DNA sequence is transcribed then it will make a new genomic RNA for progeny virus and if a part sequence of proviral DNA is transcribed then it will make mRNA and will make proteins that we are assembling now.
So after assembling gp proteins and matrix proteins the genomic RNA with reverse transcriptase, integrase, and protease are covered by capsid protein (P24) and are bulged out from the cell with the stolen lipid bilayer of the host cell membrane. There are billions of bulging out of new HIV from the cell which destroys the whole cell.
How much time this virus does take to produce AIDS?
7 to 8 years.
Is it possible that HIV-positive people do not have AIDS?
Yes, it is possible. As we discussed the co-receptor (CCR5 or CXCR4) provides a secondary attachment to the virus but in previous times some people i.e northern European descendant white population (1% of the population) were reported who be HIV positive but still didn’t get AIDS even without any treatment. The doctors were surprised but when they researched they found that this 1% population had mutant CCR5 receptors from both mother and father so the virus couldn’t make secondary attachments and couldn’t multiply and produce disease in them. About 15% of these white northern European were heterozygous for mutant CCR5 which means half of the allele from one parent was normal while half of the alleles for CCR5 were mutant and defective due to which the AIDS was not developing rapidly in that people.
And what are opportunistic diseases?
Opportunistic diseases are the diseases that attack when getting an opportunity and as discussed in AIDS the immune system is weakened and collapsed due to which these opportunistic infections occur.
Opportunistic diseases are:

- TB (tuberculosis) is an infection of the respiratory system but may damage other parts of the body.
- Lymphoma is a cancer of lymph nodes and other related lymphoid tissues.
- Pneumonia is the inflammation of the air sacs (alveoli) of the lungs.
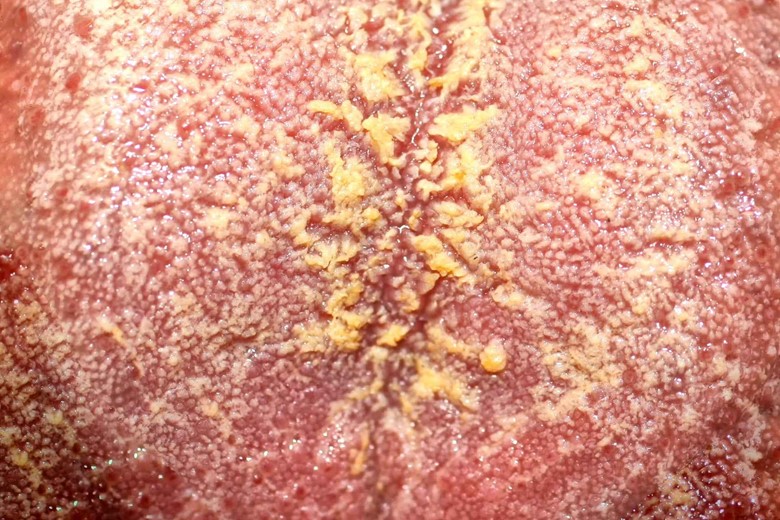
- Candidiasis affects many parts of the body like skin, nails, mucous membranes, mouth, esophagus, deeper tissues, vagina, etc.
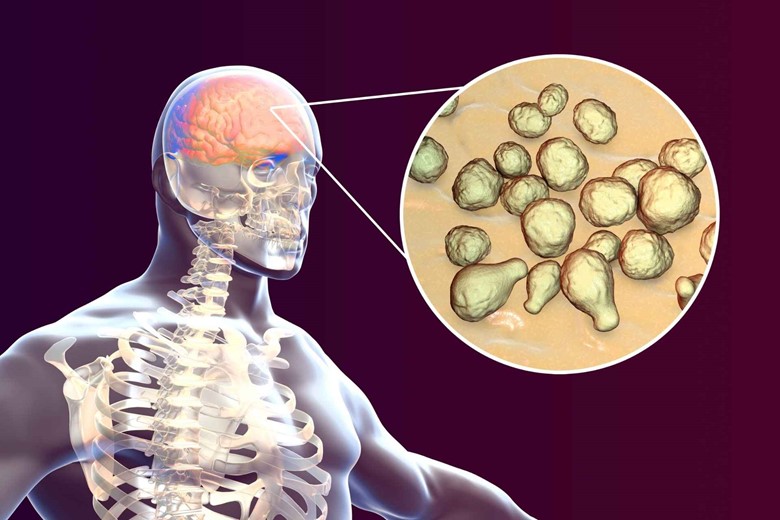
- Cryptococcosis mainly infects the lungs where it appears as pneumonia and the brain where it causes meningitis.

- Herpes simplex is caused by the Herpes simplex virus (HSV) which infects mainly the mouth and genitals where it causes small blisters.
- Toxoplasmosis is caused by the Toxoplasma gondii parasite which causes many infections but in women, it is the cause of abortion. According to the Centers for Disease Control and Prevention, more than 40 million men, women, and children in the US carry this parasite.
- Wasting syndrome is the loss of more than 10% of one’s body weight either with diarrhea or weakness and fever that lasted for at least 30 days.
What are the symptoms of AIDS?
Symptoms:
The symptoms are divided into three stages.
1. Acute infection
2. Clinical latency
3. AIDS
1. Acute infection:
- Fever
- Large tender lymph nodes
- Headache
- Rash
- Throat inflammation
- Tiredness
- Sore mouth
2. Clinical latency:
The acute stage is followed by the clinical latency stage which can last from three years to eight years on average.
- Fever
- Weight loss
- Gastrointestinal problems
- Muscle pain
3. AIDS
The third stage is AIDS which is signed by pneumocystis pneumonia, wasting syndrome, and esophageal candidiasis. Opportunistic diseases also start appearing in this stage.
How can we diagnose this disease?
The diagnosis is measured by the number of cd4 cells per cubic millimeter o blood. The following is a typical list of results.
- 500–1,200 cells per cubic millimeter are normal.
The early HIV white blood cell count may be following.
- 250–500 cells per cubic millimeter show an abnormal value and indicate HIV.
- 200 or fewer cells per cubic millimeter indicate AIDS and life-threatening opportunistic diseases.
Treatment:
- Antiretrovial therapy
- Nucleoside/nucleotide reverse transcriptase inhibitors (NRTIs) drugs like zidovudine (AZT) or tenofovir (TDF) and lamivudine (3TC) or emtricitabine (FTC).
- Dolutegravir/lamivudine/tenofovir is listed as first-line treatments for adults by the World Health Organization in 2019.
This is all about HIV and AIDS and HOW HIV REPLICATES.
Conclusion:
So the answer to “How does HIV affect/weaken your immune system” is that the cd4-positive T-helper cells are destroyed by the HIV due to which the advanced immune system is not activated resulting in a weakened immune system.
The cd4 cells (T-helper etc) have receptors for HIV due to which the virus attaches itself to the cells and invades the cells for further replication and division.




2 thoughts on “DO YOU KNOW “How does HIV affect/weaken your immune system?””
Way cool! Some extremely valid points! I appreciate you writing this write-up plus the rest of the site is also really good.
Thank you for your kind words.