Are you confused between diabetes mellitus and diabetes insipidus or diabetes insipidus and diabetes mellitus (DIABETES MELLITUS VS DIABETES INSIPIDUS OR DIABETES INSIPIDUS VS DIABETES MELLITUS)?

Yes, I want a clear answer.
Then you are in the right spot! Here I will give you a complete guide about the difference between diabetes mellitus and diabetes insipidus or diabetes insipidus and diabetes mellitus.
The name looks the same but there is a lot of difference between them.
Let’s start with “What is diabetes?”

Well, diabetes means “To go through” or “To flow through”. In other, or simple words diabetes means polyuria, while Polyuria means large urine volume.
Now diabetes has two types.
- DIABETES MELLITUS
- DIABETES INSIPIDUS
1. DIABETES MELLITUS:

As explained DIABETES means polyuria (large urine volume). While the MELLITUS means sweet so diabetes mellitus means a large volume of sweet urine.
Why do we call it “sweet”?

In our common language, we also call diabetes mellitus “sugar” because of the glucose (sugar) in urine which makes it sweet.
Let’s define diabetes mellitus:
The impaired ability of the body to produce or respond to the hormone insulin results in the abnormal metabolism of carbohydrates and a high level of glucose (sugar) in the blood.
What is meant by glucose (sugar)?
Before explaining this I want to ask “Do you know carbohydrates?”
Well, if it is explained that will be good.
Okay, let me explain to you.
Carbohydrates:

Carbohydrates are organic compounds and biomolecules whose composition is carbon, hydrogen, and oxygen with a hydrogen and oxygen ratio of 2:1, release energy upon breaking these bonds.
Their general formula is CnH2O.
Can you tell us about organic compounds?
Organic compound:
According to the modern definition “The compound of Carbon, Hydrogen, and Oxygen is called an organic compound.”
OR
The old definition is “The compounds derived from living things and can’t be prepared in a laboratory is called an organic compound.”
Classification
- Monosaccharide
- Disaccharide
- Oligosaccharide
- Polysaccharide
1. Monosaccharide:

A monosaccharide is the simplest carbohydrate with a C6H12O6 formula which cannot be further hydrolyzed into smaller units.
Example:
Glucose (sugar). (Later it will be discussed here)
Function:
Glucose is the fuel of the body which gives energy to the body for different activities in life.
2. Disaccharide:
Disaccharides are made up of two joined monosaccharides.
Example:

Sucrose, lactose, maltose.
Function:
Lactose is an important part of mammalian milk.
Disaccharide also gives energy to the body by breaking into glucose (monosaccharide).
3. Oligosaccharide:
Composed of 2 to 10 monosaccharides.
Example:
Different functions like cell recognition and cell binding.
4. Polysaccharide:
A polysaccharide is composed of many monosaccharides linked together in a chain performing important functions.
Example:


Starch, Glycogen, Cellulose, chitin (found in insects’ exoskeleton).
Function:
Starch is the reserved food of plants.
Glycogen is the reserved food of animals.
And cellulose is the structural component in plants while chitin is the structural unit of Fungi and arthropods.
Now coming back to glucose (sugar)!
Whether it is a disaccharide, oligosaccharide, or polysaccharide in food it is first broken down into monosaccharides i.e. glucose or sugar.
It means glucose gives energy to the body and serves as fuel.
Yes, that is correct.
How glucose (sugar) is controlled in the body?
That’s a good question, and our main topic is around this.
Hormones control it.
What is a hormone?
“Secretions of special cells (glands) in our body which is transported in the blood (endocrine glands) or through a special duct (exocrine glands) to the target area where cells and tissues are activated for required action.”
Okay, that’s good we are clear now and want to proceed with glucose.
Glucose is controlled by two antagonistic (opposite in function) hormones i.e
A. Insulin
B. Glucagon
A. Insulin:
(Insulin in the blood carries extra glucose to the liver)
When you eat, the glucose level rise in the blood, this should be controlled because an excess of everything causes problems. So insulin is secreted from the pancreas which increases the permeability of liver cells and muscle cells and stores the excess glucose in liver and muscle cells in the form of glycogen.
And what is Glycogen, please?

Glycogen is a polysaccharide that is a reserved food for animals as already discussed earlier.
B. Glucagon:
Glucagon is also secreted by the pancreas. When there is a need for glucose in the body, and you are working the whole day, and when you are not eating or taking any energy drink or not in the position of eating then glucose needs to be used, for this purpose, glucagon reaches the liver through the blood and converts back the glycogen to glucose keeping the balance of glucose in the blood which is 80-120 mg/dl.
I am confused about how these hormones are secreted by one pancreas?
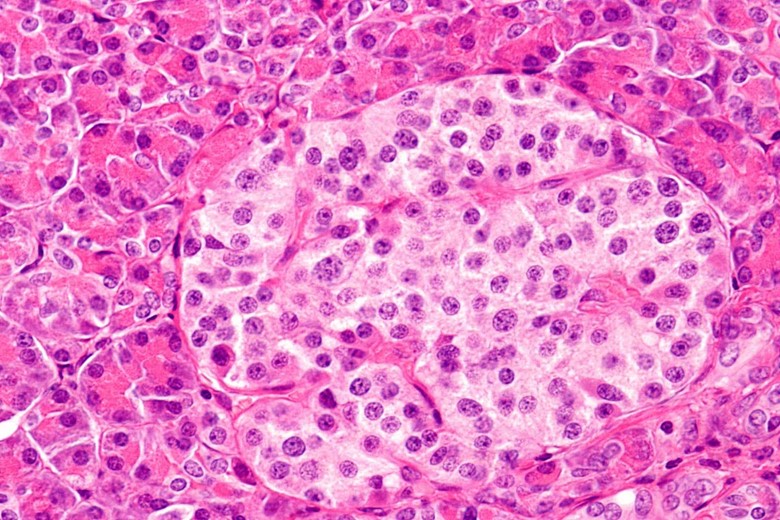
(An islet of Langerhan)
Don’t worry your confusion will be clear very soon. Actually, the pancreas has cells in the form of islets called islet of Langerhans, the name given because of courtesy to German anatomist Paul Langerhans who discovered it. The cells are:
- Beta (β) cells
- Alpha (α) cells
1. Beta (β) cells:
The beta (β) cells of Langerhans secrete insulin.
2. Alpha (α) cells:
While Alpha (α) cells secrete glucagon.
Which organ controls this balance of glucose up and down?
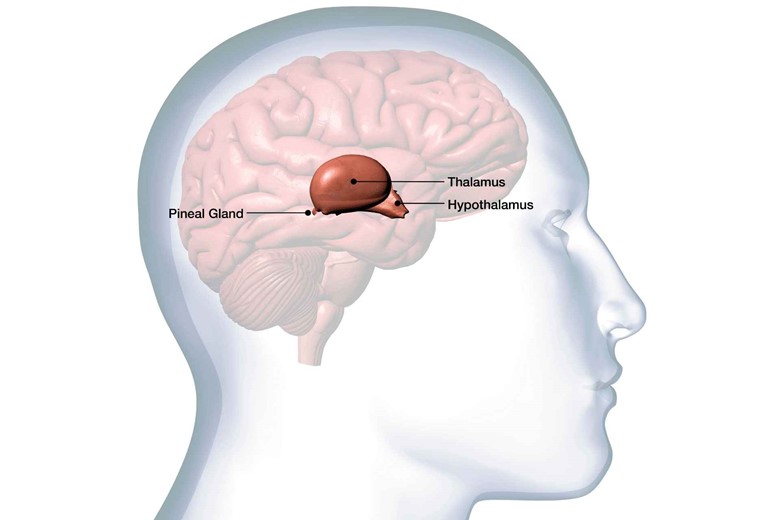
The hypothalamus, the Hypothalamus of the brain control this balance. When blood passes through the hypothalamus as it is continuously passing throughout the whole body, if there is an increase in glucose level in the blood, the hypothalamus triggers a signal to beta (β) cells of the pancreas to secrete insulin so that the insulin converts the excess glucose to glycogen into liver and muscle cells and make the concentration to the normal level i.e 80 t0 120 mg/dl (milligram per deciliter).
In contrast, if the level goes down, the hypothalamus sends a signal to alpha (α) cells of the pancreas to secrete glucagon which breaks the glycogen chain to glucose from the liver and keep the body working.
Now if there is an unbalance of these hormones then what happens to the body?
That’s our main topic here, you mean abnormality of the insulin hormone. Here we are discussing only insulin hormone because diabetes mellitus is due to insulin hormone, not glucagon.
The abnormalities are in the form of hypersecretion and hyposecretion of insulin.
Hypersecretion of insulin:
Hypersecretion is not much problem if it is not consistent. If the level rises occasionally then it is not a problem but I will discuss their symptoms so you should know their symptoms. Above 180 mg/dl is considered hypersecretion.
Symptoms:

- High Starvation because glucose is not stored.


- Sweating,

- Tiredness.
Hyposecretion of insulin:

As the name indicates secretion of insulin below than normal level is called hyposecretion.
Less than 65 mg/dl (milligram per deciliter) is considered hypoglycemia.
Very low about 30 mg/dl (milligram per deciliter) can lead to brain death because of getting no energy.
When the secretion is low then it causes a disease which we call diabetes mellitus, the topic for which we did this whole discussion.
Could diabetes mellitus be explained more, please?
Yes, sure.
When insulin is not sufficiently released then the glucose level elevates in the blood causing hyperglycemia.
Why insulin is not released sufficiently?
Let me explain this in types of diabetes mellitus to get a clear concept.
Types of diabetes mellitus
i. Diabetes mellitus type I:

In diabetes mellitus type I, insulin is not produced in the body.
Reason or cause?
The possible reason may be:

Genetic (means gene for insulin production is damaged which then cannot produce insulin)
Autoimmune (immune cells destroy beta cells of the pancreas).
ii. Diabetes mellitus type II:
In diabetes mellitus type II, insulin is produced but in a very less amount i.e. not enough for the body.
So it means there will be a high glucose level in the blood that cannot be stored in the liver or muscle cells.
Now, what will the body do with high glucose levels in the blood?

As glucose is not stored in the body so it should be eliminated in urine due to which the color of urine becomes yellowish.
Besides these symptoms, if other symptoms are also explained, that will be best for us.
Sure…!
Symptoms:

- High Starvation because glucose is not stored,

- Foot wound not healing (because of neuropathy and blood vessels damage),
- Sweating,

- Tiredness.
I hope it will be clear now.
Now it is the turn of diabetes insipidus.
2). DIABETES INSIPIDUS:

Again DIABETES means polyuria (large volume urine).

While INSIPIDUS means watery, so diabetes insipidus means a large volume of watery urine. Watery means a large amount of water in urine. Remember this is not diabetes (diabetes mellitus).
why diabetes insipidus is actually not diabetes?
Because here the glucose is not lost in the urine and it is not related to insulin rather it is related to Antidiuretic hormone (ADH) and frequent urination.
Let’s define it:
A rare disease form of diabetes resulting from a deficiency of antidiuretic (ADH) or vasopressin hormone characterized by a large amount of dilute urine (nearly 20 liters per day) and increased thirst (polydipsia).
What is antidiuretic or vasopressin and what is their function?
The antidiuretic hormone which is also called vasopressin is a water-conserving hormone and its function is to absorb more water from the last part of the nephron of the kidney to compensate for the need for water.
From where this hormone is released?
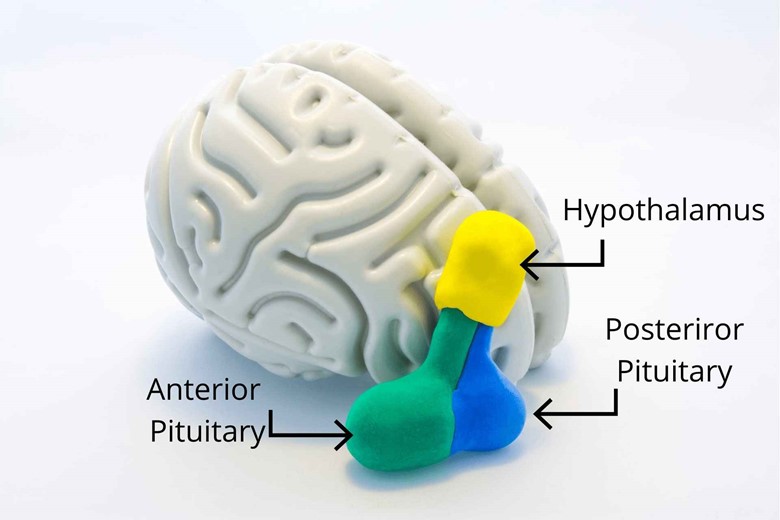
ADH is primarily synthesized in the hypothalamus and then released from the posterior pituitary gland (Adenohypophysis). The Supra optic nucleus in the hypothalamus synthesized the ADH and then sends it to the posterior pituitary gland for release.
When it is needed to secrete ADH?
When the blood becomes hyperosmolar or becomes concentrated the cells become shrink because of loss of water in urine, sweating, defecation, etc.

And the second strong reason for releasing ADH is nausea and vomiting because in vomiting water is lost which needs to be restored to normal.
The normal value of osmolarity in the blood is 300 mosml/L.
Who detects these changes in higher concentrations of solute molecules?
There are special organs near the hypothalamus in the brain called Sub fornical organs and organum vasculasim. These organs have special cells called osmoreceptors which detect the osmolarity of blood and give that data to the median preoptic nucleus while the median preoptic nucleus has a good connection with the medulla and medulla to alter and control ADH. When there is a need for ADH the median preoptic nucleus is stimulated and sends the ADH to the pituitary gland for secretion.
Can you tell us how ADH works?
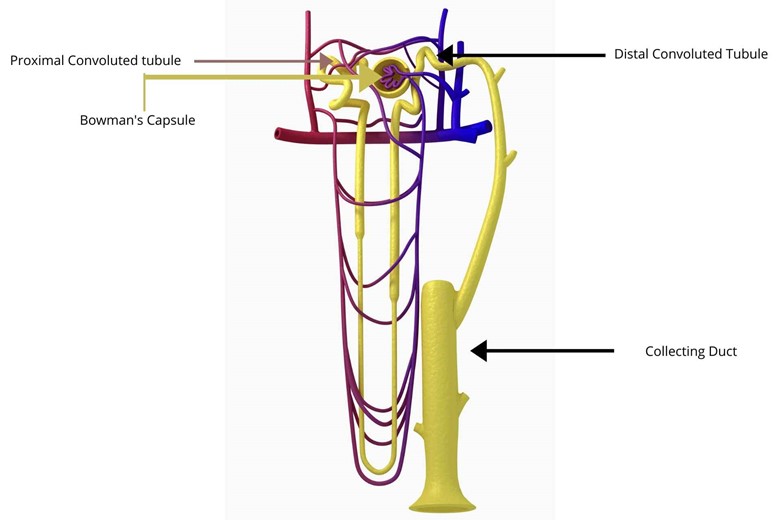
Well, this is a long phenomenon but here I am giving a short description here. The fluid moving through the last part (distal convoluted tubules, collecting tubules, and collecting ducts) of nephrons are very diluted.
The cells of the last part of nephrons are interesting if the ADH is present then it becomes permeable to the interstitium (spaces between tissues and organs) so that the water is reabsorbed to the interstitium and makes the water level normal for the body. But if ADH is not released then the cells of collecting ducts become impermeable to water so that it does not reabsorb the water from the fluid in the last part of the nephron secretes and ultimately the diluted urine will be secreted. This loss of water is called diuresis.
Why does ADH only act on distal convoluted tubules, collecting tubules, and collecting ducts of the nephron?
Because the receptor for ADH is present on these tubules which is called the serpentine receptor. The ADH released in the blood reaches the serpentine receptor in the last part of the nephron and stimulates the intracellular G stimulatory protein which in turn stimulates adrenaline cyclase which converts ATP (adenosine triphosphate) to cAMP (cyclic adenosine monophosphate) and their numbers rise. When cAMP rises it will stimulate a protein called protein kinase A. The protein kinase A phosphorylates vesicle protein (sac or vesicle-like), and this vesicle protein has special water pores or channels called aquaporin type 2 for water movement.
After phosphorylation, the vesicle protein with water pores (aquaporin type 2) and channels fuse with the lumen membrane of nephron distal tubules and become their part. It is like extra sucking pores are planted on the lumenal membrane of the nephron which reabsorbs the water into concentrated blood and makes it back to normal.
But are there, not any own permanent pores?

There is another type of aquaporin on the lumen cells of the nephron but ADH plants extra porcine for excess reabsorption to cope with the need for water.
And what type of urine will be produced?

The urine will be concentrated because water is reabsorbed by ADH leaving less water with a solute concentration greater.
Can you tell us this story in short and simple words?
In simple words, you can say that ADH or vasopressin increases the permeability of the last part of the nephron by planting pores or channels in them and reabsorbing the water from collecting ducts of the nephron releasing less concentrated urine while diabetes insipidus is due to deficiency of this hormone (ADH).
Types of diabetes insipidus:
1. Cranial diabetes insipidus:
In cranial diabetes insipidus, there is no or very little production of ADH or vasopressin through the hypothalamic posterior pituitary system.
Can you tell us what is the reason for cranial diabetes insipidus?
The reason may be:
- Infection in the Central Nervous System

- Trauma to CNS

- Tumor

- Congenital (born with abnormality)
How does ADH then affect them?
As the ADH is not produced by the hypothalamic posterior pituitary system so there will be no permeability in the last part of the nephron and the body will secrete a lot of diluted urine. The blood will become hyperosmolar or concentrated because of less reabsorption of water to it.
What are their Symptoms?
Symptoms:

- Polydipsia (excessive thirst)

- Polyuria (excretion of a large amount of diluted urine)

- Dehydration
- Increased blood osmolarity
And what is their treatment?
Treatment:
The treatment for cranial diabetes insipidus is:
Desmopressin:
which is given either in spray oral or injection form.
2. Nephrogenic diabetes insipidus:

In Nephrogenic diabetes insipidus, the ADH is produced normally but the kidney is unable to respond to ADH.
- When the receptor cells or cells of the last part of the nephron don’t respond to ADH. This condition is common in those people who are taking lithium carbonate or just lithium for depression relief which damages the cells of collecting ducts.
- When interstitial osmolarity is disturbed and the fluid is less concentrated then even the release of ADH will not reabsorb the water and will be excreted in the urine.
- Hypokalemia (low blood potassium level).
- Drugs like demeclocycline (Declomycin), ofloxacin (Floxin), orlistat (Alli, Xenical).
What are their symptoms?
Symptoms:
The symptoms may be acquired or genetic in Nephrogenic diabetes insipidus, acquired means that they are acquired and not from birth.
The most common causes are:
- Polydipsia (excessive thirst)
- Amyloidosis is a group of diseases in which abnormal protein called amyloid fibrils builds up in a tissue. Amyloid deposition in the kidney can cause nephrotic syndrome which reduces the kidney filtering ability. The symptom is the protein in the urine.
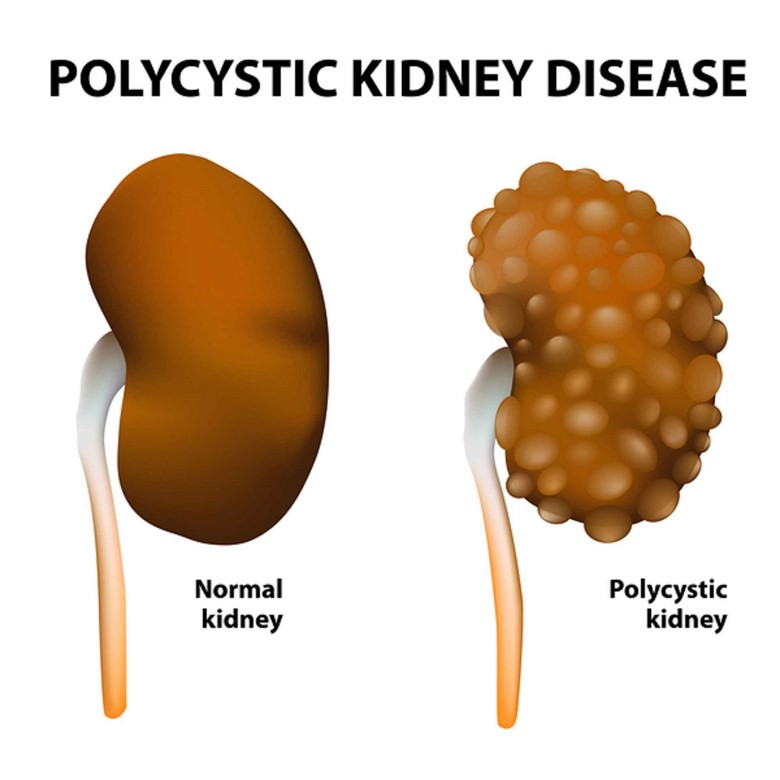
- Polycystic kidney disease (A genetic disorder in which renal tubules become abnormal in structure leading to the development and growth of cysts in the kidney).

- Electrolyte imbalance
- Renal cystic disease
Treatment:

- Thiazide diuretics are used to treat nephrogenic diabetes insipidus.
- May advise a low-salt and low-protein diet

- Non-steroid anti-inflammatory drugs.
Now can you tell us what is the difference between Cranial diabetes insipidus and Nephrogenic diabetes insipidus?
Well, in Cranial diabetes insipidus the ADH level is almost nil but the blood is hyperosmolar (concentrated) and urine is hypo-osmolar (diluted), while in Nephrogenic diabetes insipidus, only the ADH is high in concentration while the remaining situation is the same i.e concentrated blood and diluted urine.
And how can we differentiate a case if it is cranial diabetes insipidus or nephrogenic diabetes insipidus?

Very simple, just give the patient a desmopressin injection or spray, if the patient starts producing concentrated urine after the injection or spray then it must be Cranial diabetes insipidus because in Cranial diabetes insipidus the problem is nil production of ADH.

But if the patient doesn’t produce concentrated urine after desmopressin spray or injection then it will be Nephrogenic diabetes insipidus because in this case, the kidney is unable to ADH due to pathology to the kidney even the hypothalamus and pituitary gland are producing it.
But I have seen some people who drink (polydipsia) a lot of water and the results of ADH and kidneys are normal?

This is called psychogenic polydipsia. In psychogenic polydipsia, the person drinks a lot of water and produces a lot of diluted urine because the ADH doesn’t need to be secreted so there is no reabsorption of water through the last part of the nephron, though the hypothalamus, pituitary, and kidneys work normally.
How to find this condition and differentiate it from cranial and nephrogenic diabetes insipidus?
It is also very simple, just deprive the patient of water for a few hours and check if the patient is producing concentrated urine. If the patient is producing concentrated urine then this condition is psychogenic polydipsia and their systems related to water absorption are normal.
Conclusion/summary:
So what we concluded from the whole discussion is that Diabetes mellitus means the production of a large amount of concentrated urine. The concentration of urine is due to glucose (monosaccharide) in it which is sweetest in taste. The color of urine is yellowish in appearance due to the glucose in it. The condition arises from the non-production of insulin or produced in a very little amount from islets cells of Langerhans in the pancreas which is not sufficient for the body. The patient eats and feels recurring poignant hunger because the glucose is not stored in the liver which serves as energy for activities when food is not available i.e. in office work from morning to lunchtime.
The diabetes insipidus is again the production of a large amount of dilute urine which is opposite to diabetes mellitus where the urine was concentrated. This condition is due to no production of vasopressin (ADH) (Cranial diabetes insipidus) or no response of the kidney (due to some pathology) to ADH (Nephrogenic diabetes insipidus). When there is a need for water in the body the ADH is released from the pituitary gland, synthesized in the hypothalamus, and reaches to nephron of the kidney through blood where it increases the permeability of the last part of the nephron and increases the reabsorption of water to cope the need of water. But in diabetes insipidus, the patient doesn’t produce ADH or the kidney doesn’t respond to normally produced ADH so the water is not reabsorbed by the nephron and the patient secretes a lot of diluted urine.
Which glucose monitor are you using for diabetes mellitus, tell in the comment box, and also comment on what are you using for diabetes insipidus. Desmopressin spray, injection, or oral medications.
I hope this discussion has helped you. Tell me in the comment box if it helped.




6 thoughts on “DIFFERENCE BETWEEN DIABETES MELLITUS AND DIABETES INSIPIDUS”